


Introduction
This report was prepared by the World Council for Health (WCH). The report was prepared to determine whether sufficient pharmacovigilance data exists on WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellow Card Scheme to establish a safety signal on Covid-19 vaccines.
These databases are not normally used to establish the safety of an intervention. However, Covid-19 vaccines are in Phase 3 trials, and their safety and efficacy have not yet been established. The majority of those who have received the intervention (several billion people) are not being monitored by the trials. In this report, the WCH aims to use these established pharmacovigilance databases to detect if there is a concerning safety signal in those not being monitored by the clinical trials.
This report collates pharmacovigilance data about Covid-19 vaccines and other commonly administered interventions from these databases. It collates data about the types of adverse event reports linked to Covid-19 vaccines on these databases. Using data from VAERS, FAERS, and historical records, the report collates data about the rate of adverse events that have been sufficient for product recall in the past.

Purpose of Report
This report was prepared to determine if there is sufficient data on well-established, existing pharmacovigilance databases to establish a safety signal regarding Covid-19 vaccines.
Covid-19 Vaccine Development was Rushed
Covid-19 vaccine development under Operation Warp Speed was rushed. Traditionally, vaccine development takes 10 years or more before large-scale production and distribution to a wide population. With Covid-19 vaccines, the product moved from exploratory, pre-clinical trials to large-scale manufacturing in just 10 months.
Traditional Vaccine Development Timeline Compared to Potential Operation Warp Speed (OWS) Timeline
Because the development of these products was rushed, data about their safety are incomplete. In the interest of making a more complete picture of the safety of these novel products, this report collates:
1
Data from Pharmacovigilance Databases about Covid-19 Vaccines and Other Commonly Administered Vaccines and Interventions
This report collates adverse event data on COVID-19 vaccines from the following pharmacovigilance databases:
- The World Health Organization (WHO) – VigiAccess
- The US Center for Disease Control (CDC) – Vaccine Adverse Events Reporting System (VAERS)
- EudraVigilance – European Database of Suspected Adverse Drug Reaction Reports
- Medicines & Healthcare products Regulatory Agency – UK Yellow Card Reporting Site
The Covid-19 vaccine adverse event data gathered on each pharmacovigilance database is compared with the adverse event data of similar pharmacological products (other common vaccines) on the same databases when possible.
2
Data about the Types of Adverse Reactions Linked to Covid-19 Vaccines
In addition, this report examines the types of adverse reaction reports linked to Covid-19 vaccines on the above databases.
3
Data about the Rate of Adverse Events that is Sufficient for Product Recall
This report examines the parameters by which other vaccines and drugs have been recalled in the past.
This is an informational report created by World Council for Health to aid healthcare practitioners, scientists, and individual citizens in making informed decisions about Covid-19 vaccines.
The report seeks to answer the question: Are the pharmacovigilance data contained on these databases sufficient to establish a safety ‘signal’ for Covid-19 vaccines that indicates product recall?
About World Council for Health
Our Mission
The World Council for Health is a non-profit organization for the people, that is informed and funded by the people. Our global coalition of health-focused organizations and civil society groups seeks to broaden public health knowledge and sense-making through science and shared wisdom. We are dedicated to safeguarding human rights and free will while empowering people to take control of their health and wellbeing.
What we do
The World Council for Health (WCH) is a gathering of the world’s best health advocates, doctors, scientists, and innovators committed to an ongoing, transparent conversation on global health issues. This conversation is made accessible to all–governments, organiztions, and individuals looking to advocate for better health. The WCH works collaboratively with 130+ organizations in 40 countries to advance public health knowledge and sensemaking. Together, we take action to defend health freedom and promote healthy lifestyles.
Who we are
Founded in 2021, World Council for Health is a non-profit initiative supported by EbMCsquared CiC, a community interest organization. World Council for Health is guided by its international Coalition Partners, Steering Committee, Volunteers, and Support Staff.
Our vision
We believe in a healthy world, where everyone enjoys information transparency, access to proven medicines, and real action in the face of disease – while respecting each individual’s personal health decisions, without fear of discrimination or persecution. We believe in a world where we keep our water and air clean, food uncontaminated, and families together.
Our partners
Our coalition partners bring expertise in science, medical care, legal protection, and community organizing skills to help us achieve our goals.
Our Values
Freedom
Freedom is the right to say, think and do whatever you want to do without being limited. Everyone has this innate human right. It is our responsibility to use it wisely.
Community
The strength of the World Council for Health is in its approach to collaboration. We are powered almost entirely by volunteers in our growing number of committees made up of scientists, medical practitioners, lawyers, activists, and patients. We work across borders dissolving barriers through international coalition partnerships united for the protection of humanity.
Integrity
We value honesty, self-awareness, and a strong moral compass. These together make up integrity and it is important that we hold these in our hearts in order to create the foundations for change.
Transparency
World Council for Health is committed to clear and open communication. Many of the issues we see in the world today are a result of a lack of transparency and accountability, as well as censorship of important truths. We live stream out weekly General Assembly meetings and other events to the public so that anyone can tune in, listen and learn or rewatch later.
Empowerment
Through education and ethos, we empower people to step away from fear and engage more fully in living life. We do this by providing them with the resources to optimize their health and wellbeing so we might be able to step into our collective power.
Methodology
This report was designed to see whether or not there is sufficient evidence on the WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellowcard databases to establish a safety signal about Covid-19 vaccines. In ordinary circumstances, Phase 3 and 4 trials would establish the safety and efficacy of a pharmaceutical product. However, these trials are not complete for Covid-19 products. The products have been administered to a wide population that is not being monitored by the clinical trials. The need exists, therefore, to look at all available evidence to establish the safety of these products and how they might be impacting those who have taken the product but are not being monitored by the clinical trials.
The Need to Examine All Evidence
Traditionally, pharmacovigilance data from passive reporting systems (such as those highlighted in this report) are only used to detect safety signals for rare adverse events that may have been missed in clinical trials. However, several key factors arising from the unique acceleration of Covid-19 products for use in the general public highlight the need to examine all available evidence to establish the suitability of these products for use in humans. These include:
- The safety of Covid-19 products has not been established through the completion of Phase 3 and Phase 4 clinical trials
- The dubious, waning, and decreasing efficacy of Covid-19 products
- Covid-19 products do not function like other similar vaccine products. (i.e. they do not prevent someone from contracting, spreading, or becoming ill with the virus)
- Covid-19 products are being employed on billions of people, including children, during the clinical trial phase. The vast majority of these people are not being monitored
- A greater understanding of the risks associated with Covid-19 illness
- The availability of other safer products to mitigate harm from the disease
- Pfizer’s 6-month trial data (that followed up on the original trial data on which the products were authorized), failed to show a reduction in all-cause mortality in the vaccinated group. This could indicate that any benefit gained through vaccination may be negated by adverse events including death
Method
This report was completed as follows:
- We looked at each database–WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellow Card Scheme–and documented how many adverse events were related to Covid-19 vaccines.
- We looked at other similar products (other commonly administered vaccines, where possible, and other commonly administered pharmaceutical products) and documented how many adverse events were related to those products.
- We normalized these, where possible, to the number of adverse events per individual who had received each intervention, and contrasted the number of adverse events related to Covid-19 vaccines with the number of adverse events related to similar products.
- In addition, where possible, we examined the trends in reports of adverse events and deaths over the past two years.
- We note adverse event reports in age groups for which the Covid-19 products have not been authorized.
- We examine the most commonly reported adverse events on each database by type.
- We examine whether pharmacovigilance reports are over-reported or under-reported.
- We note historical cases where adverse event reports have led to recalls of pharmaceutical products.
Pharmacovigilance at a Glance

pharmacovigilance noun
phar·ma·co·vig·i·lance |
Medical Definition of pharmacovigilance
: the monitoring, evaluation, and prevention of adverse effects associated with the administration of medicines
What is Pharmacovigilance?
Pharmacovigilance is a pharmaceutical science, also known as drug safety. The goal of pharmacovigilance is to collect, assess, and monitor data and, ultimately, to prevent adverse events related to pharmaceutical products. Most data in pharmacovigilance is gathered through adverse event (AE) reporting, but it is also collected in other ways.
Pharmacovigilance databases containing adverse events are an inexpensive and accessible way to detect safety concerns around pharmaceutical products.
How Pharmacovigilance Data is Gathered
Adverse Events Reports
Pharmacovigilance data is commonly gathered through adverse event reporting. Generally, adverse events reports are made by:
- An individual who has experienced an adverse event
- A healthcare practitioner who suspects an adverse event in a patient
- Organizations who create reports from patient support programs
- Pharmaceutical companies in the form of clinical or post-marketing studies
- Literature reviews
- Media reports
Studies
Pharmacovigilance data may also be gathered through other studies including:
- Retrospective studies
- Cohort studies
- Clinical studies
- Post-marketing studies
- Literature reviews
Reports
Some pharmacovigilance data is sourced from reports from:
- Patient support organizations
- Media
- Pharmaceutical companies
- Drug regulatory bodies
- Government agencies
Population Data
Pharmacovigilance data may also be from sourced population data such as:
- Statistics
Medical Definition of adverse event
: a harmful effect associated with the use of a medical product including but not limited to: death, life-threatening injury, hospitalization, disability, congenital defects, and other serious medical events
severe adverse event noun
se·vere ad·verse e·vent
Medical Definition of severe adverse event
: a harmful effect associated with the use of a medical product that significantly limits daily function including but not limited to: death, life-threatening injury, hospitalization, disability, congenital defects, and other serious medical events
Pharmacovigilance Databases Around the World
Many countries around the world have their own reporting systems for adverse events. Some databases gather reports from around the world, and some databases gather reports solely from their country of origin. All of them have different methods of reporting. Reports may be:
- Made by healthcare practitioners on behalf of patients
- Made by individuals experiencing an adverse event
- Vetted by public health authorities
- Vetted by regulatory officials
For this report, we will focus on pharmacovigilance data sourced from Adverse Event Reports on some of the largest and most well-established databases in the world: WHO VigiAccess, VAERS, EudraVigilance, and UK Yellowcard Reporting System.
Pharmacovigilance Data Establishes Signals
Reports made on pharmacovigilance databases do not establish causation. One important part of the science of drug safety is a process known as ‘Signal Detection’ in which a variety of techniques are employed to determine if reports point to a possible causal relationship between the product and the adverse events being reported. A possible causal relationship established through this process is known as a ‘signal.’ If a signal is detected, further in-depth investigation is required.
List of Pharmacovigilance Databases
Table 0: Vaccine adverse event or reaction reporting databases
Covid-19 vaccines are a new type of therapy, and their safety is still being understood; therefore, it is especially important to report serious side effects. Depending on where you are in the world, there are various databases set up to record adverse drug reactions:
[ninja_tables id=”6546″]
Learn more about vaccine adverse event reporting databases
WHO VigiAccess
At a Glance
Launched in 2015 by the WHO, VigiAccess is an international database of reported potential adverse events related to medicinal products. Some of their stated goals are to “enable individual countries to be alerted to patterns of harm emerging across the world” and “to analyse reports of suspected harm caused by medicines, to find what are known as “signals” of potential adverse drug reactions.”
How Reports are Made
Reports to VigiAccess are made by members of the WHO Programme of International Drug Monitoring (PIDM). Created in 1968, the WHO PIDM members include national pharmacovigilance centres and drug regulatory bodies from 170 countries who collaborate to monitor and identify harms caused by medicines. This collaboration covers about 99% of the world’s population.
Important Notes
- Covid-19 vaccine adverse event reports on VigiAccess encompass all Covid-19 vaccines
- Other vaccine adverse event reports are for the active ingredient and often include multiple brand names
- VigiAccess does not contain contextual data such as how many people have taken a product, how long it has been on the market, or disparities in reporting. Some of this data is sourced elsewhere for this report
- Reports are collected from 1968 or later
The Data
VigiAcess Data for Covid-19 Vaccines and Tuberculosis Vaccines
Source: vigiaccess.org
Table 1: Contextual Data of Covid-19 and Tuberculosis Vaccines on VigiAccess
[ninja_tables id=”75862″]
Discussion
The tuberculosis vaccine has been administered to the highest percentage of the world’s population, more than any other vaccine. 88% of 1 year olds have been immunized against tuberculosis. Some 4 billion individuals have received the vaccine. VigiAccess reports around 37 thousand adverse event reports relating to the tuberculosis vaccine.
At least one dose of the Covid-19 vaccine has been administered to 65.7% of the world’s population or approximately 5.1 billion individuals. VigiAccess reports around 3.8 million adverse events reports relating to the Covid-19 vaccine.
Table 2: Other Vaccine Adverse Event Data on VigiAccess
[ninja_tables id=”75964″]
*** Percentage of current world population ***
Discussion
For common vaccines that have been distributed to the vast majority of the world’s population, we see a range of adverse event reports numbering between 2000 and 100 000 on VigiAccess.
For the Covid-19 vaccines, which have currently been administered to around 65% of the world population, there are over 3.7 million reports of adverse events on VigiAccess.
Comments
VigiAccess shows a number of adverse events that is unprecedented on the database for any other pharmaceutical product or vaccine. The total reports of adverse event reports cannot be compared directly because of the lack of contextual data discussed earlier. However, given that other similar products have been widely distributed on a global scale in comparable numbers, the magnitude of disparity is cause for grave concern. This data is particularly relevant given that Covid-19 vaccines are being widely distributed, are still in clinical trials, and must be scrutinized using all available evidence.
In Table 2, we see 37 335 adverse event reports from an estimated 4 billion individuals who have received the tuberculosis immunization and over 3.7 million reports from an estimated 5.1 million individuals who have received the Covid-19 vaccine. Correcting for the difference in the number of individuals who have received the two vaccines, we see an 80-fold increase in the number in adverse events reported to VigiAccess for the Covid-19 vaccine.
Given VigiAccess’ stated purpose–to analyse reports of suspected harm caused by medicines, to find “signals” of potential adverse drug reactions–immediate investigation and urgent action are required from the World Health Organization.
CDC VAERS
At a Glance
Vaccine Adverse Event Reporting System (VAERS) was established in 1990 and co-managed by the United States Centers for Disease Control and Prevention (CDC) and the United States Food and Drug Administration (FDA). The system is designed to be an early warning system for safety concerns related to US-licensed vaccines. VAERS inputs and analyzes reports of adverse events that occur after a vaccination.
Some of the stated purposes of VAERS are to “detect new, unusual, or rare vaccine adverse events,” “assess the safety of newly licensed vaccines,” and “provide a national safety monitoring system that extends to the entire population for response to public health emergencies, such as large-scale pandemic influenza vaccination programs.”
How Reports are Made
Any individual who has experienced an adverse event following a vaccine may report to VAERS. In addition, healthcare practitioners are required to report prescribed events that occur in their patients after vaccination, and vaccine manufacturers are required to report all adverse events that come to their attention. It is a passive reporting system which relies on individuals to self-report or healthcare providers to report on their behalf.
Important Notes
- VAERS is a passive surveillance system
- VAERS does not contain contextual data such as how many people have taken a vaccine, how long it has been on the market, or disparities in reporting. Some of this data is sourced elsewhere for this report
- VAERS Reports are from 1990 to the present
- Covid-19 vaccine data on VAERS encompasses Moderna, Pfizer, and Janzen vaccines
- It is a federal offence in the United States to submit a false VAERS report
- VAERS has been used as a pharmacovigilance tool in the past for intussusception of vaccines (a small number of anamolous reports in VAERS related to the Rotavirus vaccine in children led to intussusception)
Data
VAERS Data: Percentage of Total Adverse Event Reports by Vaccine Type
Discussion
Over 50% of total adverse event reports made on VAERS, that is reports made for ALL vaccines since 1990, are attributed to COVID-19 vaccines.
Table 3: Contextual Data of Covid-19 Vaccine and Measles, Mumps, Rubella Vaccine on VAERS
[ninja_tables id=”76502″]
Discussion
Over 50% of total adverse event reports made on VAERS, that is reports made for ALL vaccines since 1990, are attributed to COVID-19 vaccines.
OpenVAERS is a project that allows browsing and searching of VAERS reports without the need to compose an advanced search. OpenVAERS has generated the above graphs and tables regarding Covid-19 adverse events reports and total death reports which are updated regularly.
The second table above shows the mean number of deaths reported on VAERS from 1990 – 2020 at 122, followed by an alarming and unprecedented spike in death reports for 2021 and 2022.
From these data representations, we can observe an alarming trend in the number of deaths reported to VAERS per year. Starting in 2020 and continuing to 2022, we see a dramatic and unprecedented spike in deaths reported to VAERS. Currently of the over 37 000 deaths reported to VAERS since 1990, 27 968 are related to Covid-19 products. A death in close proximity to a vaccine indicates a more likely causal relationship. As illustrated in the second to last graphic above, a vast majority of reports are made within 3 days of the vaccine being administered.
Covid-19 VAERS Reports by Age
Source: https://wonder.cdc.gov/controller/datarequest/D8;jsessionid=F9E61FE2A2B457AD46D5FC21F667
Discussion
There are 209 reports of adverse events on VAERS for children under 2. These vaccines have not been authorized for these age groups. There are an additional 1499 reports in the 2 – 5 year old group, many of which are likely in children for whom the vaccine has not been authorized. These may be related to exposure to the product in-utero, via breastfeeding, or being administered to children for whom the product is not authorized.
Comments
VAERS data shows an overwhelmingly large proportion of adverse events reports relating to the Covid-19 vaccine with over 50% of total reports since 1990 being attributed to the vaccine. Though, for many reasons, the adverse event reports of individual vaccines cannot be compared directly, the magnitude of the disparity in adverse events and deaths is indicative of a cause for concern. As shown in Table 3, we see a 10 fold difference in the number of adverse event reports for the MMR vaccine and the Covid-19 vaccine. In addition there is a 169 fold increase in reported deaths to VAERS after Covid-19 vaccination when compared to the flu vaccine and a 56 fold increase in adverse event reports on VAERS after Covid-19 vaccination when compared to the flu vaccine. Most deaths and adverse events occurred days after vaccination, making a causal relationship more likely. Given that Covid-19 vaccines are novel and still in clinical trials, VAERS data is sufficient to establish a concerning safety signal.
The reports on VAERS that occurred in children in age groups that have not been authorized to receive the vaccine are extremely concerning. This indicates the possibility of adverse events obtained in utero, from breastfeeding or administering the vaccine to age groups for whom it has not been authorized.
Given VAERS stated objectives–to detect new, unusual, or rare vaccine adverse events, to assess the safety of newly licensed vaccines, and to provide a national safety monitoring system that extends to the entire population for response to public health emergencies, such as large-scale pandemic influenza vaccination programs–immediate investigation and urgent action are required from the CDC and the FDA.
EudraVigilance
At a Glance
EudraVigilance – European database of suspected adverse drug reaction reports is a pharmacovigilance database for gathering and analysing suspected adverse reaction data primarily from the European Economic Area (EAA). EudraVigilance is part of the European Medicines Agency which is tasked with evaluating, supervising and monitoring the safety of medicines in the EU.
EudraVigilance seeks to gather information “on suspected adverse reactions to medicines which have been authorised or being studied in clinical trials in the EEA” that “enables the early detection of potential safety issues.”
How Reports are Made
Reports on EudraVigilance are made electronically by sponsors of clinical trials, marketing authorisation holders, and national authorities.
Important Notes
- Adverse events reports are separated by brand, but collated for the purposes of this reports
- Data from EudraVigilance is analysed by regulatory authorities across the EEA, the European Medicines Agency and pharmaceutical companies
- Covid-19 vaccine uptake in individual European countries varies dramatically with Malta having the highest vaccination rate (248 doses per 100 people) and Bulgaria have the lowest vaccination rate (63 doses per 100 people)
Data
Individual Cases of Adverse Events Identified in EudraVigilance for Covid-19 Vaccines
Source: https://dap.ema.europa.eu/analytics/saw.dll?PortalPages&PortalPath=%2Fshared%2FPHV%20DAP%2F_portal%2FDAP&Action=Navigate&P0=1&P1=eq&P2=%22Line%20Listing%20Objects%22.%22Substance%20High%20Level%20Code%22&P3=1+40983312
Discussion
The total number of individual adverse event cases identified in EudraVigilance are as follows: Covid-19 MRNA Vaccine Moderna – 294 772; Covid-19 MRNA Vaccine Pfizer-BioNTech (Tozinameran) – 956 913; Covid-19 Vaccine Astrazeneca – 488 769; Covid-19 Vaccine Janssen – 59 751; Covid-19 Vaccine Novavax – 756. The total number if individual adverse events cases identified for all Covid-19 vaccines on EudraVigilance is over 1.8 million.
There are over a thousand of cases reported in 0 – 2 years category, an age group for which the vaccines are not authorized. This potentially indicates infants and children are experiencing adverse events related to in-utero exposure, breastfeeding, and/or administered to individuals for whom the products are not authorized.
The total number of people vaccinated in EU/EEA countries is 341 628 772 or approximately 75.4% of the population.
Individual Cases of Adverse Events Identified in EudraVigilance for Measles Vaccines
Discussion
On the EudraVigilance database, the total number of individual adverse event reports are as follows: Measles, Mumps and Rubella Vaccine (LIVE) – 36 947; Measles Vaccine (LIVE) – 592; Measles and Rubella Vaccine (LIVE) – 116; Measles, Mumps, Rubella and Varicella Vaccine (LIVE) – 11 258. The total number of adverse events potentially relating to a vaccine containing a measles inoculation on EudraVigilance is 48 913.
In 2018, around 90% of European children were vaccinated for measles as part of measles, mumps, rubella vaccine.
Table 4: Contextual Data of Covid-19 and Measles Vaccine: EudraVigilance
[ninja_tables id=”76608″]
Discussion
Around 90% of Europeans have been immunized for Measles. Of the approximate 673.2 million individuals who have received the Measles Vaccine in Europe, there have been a total of 48 913 adverse event reports made on EudraVigilance.
Around 341 million European individuals have been vaccinated against Covid-19. From these, 1.8 million adverse event reports have been made on EudraVigilance.
Comments
EudraVigilance data shows a number of individual case reports that are unprecedented on the database for any other pharmaceutical product or vaccine. Though the total number of adverse event reports cannot be compared directly with other products, this data must be considered given that Covid-19 vaccines are in general distribution, still in clinical trials, and must be scrutinized using all available evidence. Given that other similar products have been similarly widely distributed across Europe, the magnitude of the disparity in total individual case reports for Covid-19 vaccines on EudraVigilance is cause for grave concern.
In Table 4, we see 48 913 individual EudraVigilance reports linked in some way to the Measles vaccine of the approximate 673 million individuals who have received the vaccine in Europe. It is possible, however, that any amount of these might be attributable to other inoculations contained in the same vaccine. We see 1.8 million individual EudraVigilance reports associated with the Covid-19 vaccines of the approximate 341 million individuals who have received the vaccine. Correcting for the difference in the number of individuals who have received each vaccine, there is an over 70-fold increase in the number of individual adverse events reported to EudraVigilance for the Covid-19 vaccine. Given that Covid-19 vaccines are in clinical trials, EudraVigilance Data is sufficient to establish an alarming safety signal for these products.
The over 1000 reports of adverse events that occurred in children for whom the vaccine has not been authorized indicates the need for immediate and urgent action.
Given EudraVigilance’s objectives–to gather information “on suspected adverse reactions to medicines which have been authorised or being studied in clinical trials in the EEA” that “enables the early detection of potential safety issues”–immediate and urgent action are required from all concerned European authorities.
UK Yellow Card Scheme
At a Glance
The UK Yellow Card scheme is run by the Medicines & Healthcare products Regulatory Agency (MHRA). The system collects and monitors data on adverse medical incidents or side effects relating to medical products such as medicines, vaccines, blood products, herbal products, and medical devices.
The scheme aims to “identify issues which might not have been previously known about,” and to “provide an early warning that the safety of a product may require more further investigation.” The MHRA states that it will “if necessary, take action to minimise risk and maximise benefit to the patients.”
How Reports are Made
Reports are made to the Yellow Card Scheme voluntarily by patients, parents, or caregivers and by healthcare professionals. Manufacturers are legally required to report problems with healthcare products to the MHRA.
Important Notes
- A report on the UK Yellow Card System implies a correlation between the vaccine and the adverse event, not the cause
- There is currently no Yellow Card data available for vaccines other than the Covid-19 vaccine
- The total numbers of adverse reactions for the Covid-19 vaccines are available in the weekly report supplied by the MHRA
The Data
Adverse Event Reports Received in the UK: Yellow Card Data
Total Number of Reports
[ninja_tables id=”76611″]
Total Number of Individuals Who have Received a Vaccine by Country
[ninja_tables id=”76629″]
Discussion
In the UK, over 53 million individuals have received at least one dose of the Covid-19 vaccine. The UK Yellow Card scheme currently documents over 450 000 reports of adverse reactions.
Yellow Card data for other vaccines is currently not available on the Yellow Card Website.
Interactive Drug Analysis Profile: Yellow Card Data for Paracetamol
Discussion
Above is the Yellow Card data for adverse reaction reports relating to paracetamol (acetaminophen). Paracetamol is one of the most commonly used medications in the UK. Millions of individuals in the UK have taken this medication for several decades. The above report shows 25 158 reactions and 585 deaths associated with its use since 1964.
Comments
The Yellow Card Scheme shows over 450,000 yellow card reports related to the Covid-19 vaccines. Though the data for other vaccines is not available on the website, the data for paracetamol, a medication in widespread use for several decades in the UK, shows only a fraction of the reports (~25 000 since 1968) on the Yellow Card Scheme. Though these cannot be used in direct comparison, the magnitude of the disparity is cause for concern. Given that the Covid-19 products are still in clinical trials, all evidence should be used to assess their safety. The UK Yellow Card data is sufficient to establish a safety signal for these products.
Given the UK Yellow Card Scheme’s objectives–to identify issues which might not have been previously known about and to provide an early warning that the safety of a product may require more further investigation and to take action to minimise risk and maximise benefit to the patients if necessary–immediate and urgent action are required.
Amount and Types of Adverse Events Reported: All Databases
What Kind of Adverse Events are Related to Covid-19 Vaccines?
There are a wide variety of adverse events reported on the databases examined in this report: WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellow Card Reporting System. They range in severity from minor such as pain at the injection site to major events like cardiac arrest, strokes, myocarditis, and death.
Table 5: Common Types and Total Number of Adverse Events: VigiAccess, EudraVigilance, UK Yellow Card Scheme
[ninja_tables id=”76658″]
*** For this report, investigations were not considered. ***
Discussion
Table 5 lists the most common reactions to Covid-19 vaccines by reaction group in VigiAccess, EudraVigilance, and UK Yellow Card Scheme.
In VigiAccess, the five most common reports by reaction group from most to least are as follows:
- Nervous System Disorders – ~ 1 500 000
- Musculoskeletal and Connective Tissue Disorder – ~ 1 000 000
- Gastrointestinal Disorders – ~ 691 000
- Skin and Subcutaneous Tissue Disorders – ~ 477 000
- Vascular Disorder – ~193 000
In EudraVigilance, the five most common reports by reaction group from most to least are as follows:
- Nervous System Disorders – ~ 746 000
- Musculoskeletal and Connective Tissue Disorder – ~ 543 000
- Gastrointestinal Disorders – ~ 344 000
- Infections and Infestations – ~ 220 000
- Skin and Subcutaneous Tissue Disorders – ~ 213 000
In UK Yellow Card Scheme, the five most common reports by reaction group from most to least are as follows:
- Nervous System Disorders – ~ 285 000
- Musculoskeletal and Connective Tissue Disorder – ~ 175 000
- Gastrointestinal Disorders – ~ 135 000
- Skin and Subcutaneous Tissue Disorders – ~ 101 000
- Reproductive System and Breast Disorders – ~ 57 000
Common Covid-19 Vaccine Adverse Event Outcomes: VAERS
Source: wonder.cdc.gov/
Table 6: Common Covid-19 Reactions by Type: VAERS
[ninja_tables id=”76656″]
Source: vaersanalysis.info/2022/05/14/vaers-summary-for-covid-19-vaccines-through-5-6-2022/
Discussion
Over 54% of adverse events reported to VAERS are attributed to the Covid-19 vaccine including death, life-threatening injury, permanent disability, congenital anomalies/birth defects, hospitalizations, emergency room visits, doctor’s office visits, and others.
Table 6 lists some of the most commonly reported reactions on VAERS to the Covid-19 vaccine. These are (from most to least):
- Arthritis and Arthralgia/Joint Paint
- Anaphylaxis
- Venous Thromboembolism
- Myocarditis/Pericarditis
- Stroke
- Convulsions/Seizures
There are over 28 000 deaths, over 75% of all deaths reported to VAERS since 1990, associated with the Covid-19 vaccine.
Comments
Table 7: 3 Most Common Reports by Reaction Group: VigiAccess, EudraVigilance, and UK Yellow Card
[ninja_tables id=”76707″]
Nervous System Disorders, Musculoskeletal and Connective Tissue Disorders, and
Gastrointestinal Disorders are the 3 most commonly reported reaction groups on VigiAccess, EudraVigilance, and UK Yellow Card Scheme.
Arthritis and Arthralgia/Joint Pain, Anaphylaxis, Venous Thromboembolism, Myocarditis/Pericarditis, Stroke and Convulsions/Seizures are some of the most commonly reported adverse events on VAERS.
The following number of reports involving death related to Covid-19 vaccines are as follows:
Table 8: Number of Deaths Reported by Database: Covid-19 Vaccines
[ninja_tables id=”76708″]
How Many Adverse Events is Too Many?
Active vs. Passive Surveillance
Pharmacovigilance databases such as VigiAccess, EudraVigilance, VAERS, and UK Yellow Card Scheme rely on passive reporting from healthcare providers, pharmaceutical companies, and individuals.
Passive reporting or passive surveillance of adverse events means that the onus of reporting falls on the individual (and/or their healthcare provider) who received a vaccine or other pharmaceutical product. If an adverse event is noted, the individual or healthcare provider may voluntarily report.
Active reporting or active surveillance of adverse events means that a pharmaceutical company or healthcare body is actively collecting adverse event reports through careful and comprehensive monitoring procedures.
Adverse Events on Pharmacovigilance Databases are Under-Reported
Passive surveillance, such as the pharmacovigilance databases studied in this report, result in significantly less adverse event reports than active surveillance reporting. In a study comparing active and passive surveillance of adverse events, 8.8% of those under active surveillance reported and adverse event, while only 0.1% of those under passive surveillance reported an adverse event. That is an 88 fold difference in the number of reports for that particular study. The WHO also notes that passive surveillance “makes it difficult to ensure completeness and timeliness of data collection.” Studies of new pharmaceutical products normally require active surveillance of adverse events during the clinical trial phase. The number of adverse events documented during active surveillance is universally higher than what is passively reported to pharmacovigilance databases later. The actual number of adverse events that occurred in temporal relation to Covid-19 vaccines would be much higher than is revealed by the data in these pharmacovigilance databases.
As stated earlier in this report, an adverse event report is not indicative that the vaccine caused an event, simply that it was related. However, the likelihood that a product caused an adverse event increases as the time between administration of a product and the adverse event decreases. VAERS data reveals a close temporal relationship between the administration of the Covid-19 vaccine and the subsequent adverse event with a majority of adverse events happening within just 2 days of receiving the vaccine. This indicates a more likely causal relationship.
The Unique Case of Covid-19 Vaccines
Operation Warp Speed
When Covid-19 emerged as a novel virus in 2019, little was known about its virulence and what its impacts would be on the general population. Early models overestimated the morbidity and mortality of the illness, and, as a result, “Operation Warp Speed” was introduced to accelerate the development of a vaccine and other therapeutics for the novel virus. Several government agencies collaborated to develop, study, manufacture, and distribute Covid-19 vaccines. Operation Warp Speed meant that vaccine studies were accelerated and that the products were pushed to market while still in clinical trials.
ALL Covid-19 Vaccines are in Phase 3 Trials
On August 23, 2021, the US Food and Drug Administration (FDA) approved the first Covid-19 vaccine. Many other countries health authorities followed suit soon after. Prior to that, the vaccines were administered to billions of people under emergency use authorization. Many people understood that ‘approval’ meant that vaccines were no longer experimental. That is not true. ALL Covid-19 vaccines, including those that are approved, are still in Phase 3 clinical trials.
What are Phase 3 Clinical Trials?
According to the FDA, Phase 3 trials:
- Involve 300 – 3000 volunteers
- Last 1 to 4 years
- Are designed to establish efficacy and monitor adverse reactions
- 25 – 30% of products will make it to the next phase of clinical trials
The efficacy and safety of Covid-19 vaccines has, therefore, not been established. In addition, the number of volunteers recruited for Phase 3 trials of this product is highly unusual.
What are Phase 4 Clinical Trials?
According to the FDA, Phase 4 trials:
- Involve several thousand volunteers
- Last 10 – 15 years
- Are designed to establish safety and efficacy
Covid-19 vaccines have not yet entered Phase 4 trials.
The 1976 Swine Flu: A Case of a Rushed Mass Vaccination Campaign
In February 1976, an investigation was launched into the mysterious death of an American Private who died during a basic training exercise. CDC tests revealed that Private David Lewis had contracted a strain of swine flu. Subsequently 11 other soldiers tested positive for the virus while hundreds of others tested positive for antibodies. Alarming headlines appeared in newspapers across the country, and, the CDC Director, citing a “strong possibility” of a pandemic, recommended an unprecedented plan of mass vaccination of US citizens.
Though no further evidence emerged that the virus was problematic, the CDC and then President Gerald Ford adopted a ‘better safe than sorry’ approach, and began a mass vaccination campaign for the swine flu. When reports emerged of suspected adverse reactions, including heart attacks, Guillain-Barre syndrome and 53 reported deaths, citizens began doubt the safety of the vaccine. Coupled with the fact the pandemic did not materialize as predicted, the government halted the mass vaccination program on December 16.
Key Lessons from the 1976 Swine Flu
Though the landscape of 2022 is very different, the following key insights from the mass swine flu vaccination campaign should be highlighted:
- It is essential for scientists and policy makers to re-evaluate information derived from early models as real-time information emerges about a suspected pandemic
- A ‘better safe than sorry’ approach is confounded by the issue that the evidence does not yet exist to make the statement that a rushed vaccination is safer than exposure to a virus about which little is known
- Reports of as few as 50 deaths linked to the swine flu vaccination were enough to shut down the program completely
- Natural immunity must be considered
- Responses to any suspected pandemic must align with the best available evidence about the nature of the threat and not be guided by politics, media, and emotions of the general public
Major Drug and Vaccine Recalls in History
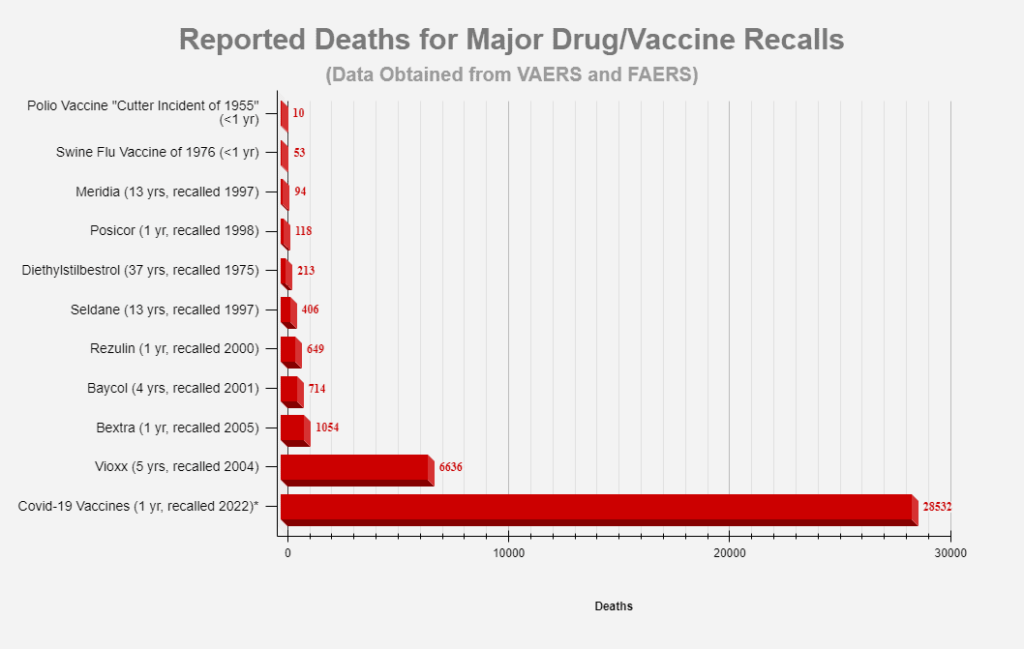
When a concerning number of adverse events or deaths is noticed in pharmacovigilance reports, governing bodies may recall a previously authorized or approved product. The following graph shows the number of deaths reported to VAERS or FAERS before a product was recalled.
Source: vaersanalysis.info/2022/05/14/vaers-summary-for-covid-19-vaccines-through-5-6-2022/
The Polio Vaccine was recalled in less than 1 year after 10 reported deaths, the Swine Flu Vaccine was recalled in less than 1 year after 53 reported deaths. The Covid-19 vaccine, with over 28 000 associated reports of death, has not been recalled.
Signal Detected
Table 9: Total Adverse Events per Pharmacovigilance Database
***Yellow Card data excluded***
Discussion
Across all databases, Covid-19 vaccines show an alarming number of adverse events and death reports when compared to other commonly administered vaccines.
Comments
There is concerning safety signal regarding Covid-19 vaccines detected on all databases examined in this report.
Conclusion
This report sought to look at pharmacovigilance data from VigiAcess, VAERS, EudraVigilance, and UK Yellow Card for Covid-19 vaccines. The aim was to determine if the data on these databases was sufficient to establish a safety signal about these products. We conclude the following:
Data from Pharmacovigilance Databases about Covid-19 Vaccines vs. Other Commonly Administered Vaccines and Pharmaceutical Products
- All pharmacovigilance databases examined in this report reveal a number of adverse events reports linked to Covid-19 vaccines that are between ten times and 169 times more than what is observed in other commonly administered products
- There are several thousand reports of adverse events in children for whom the Covid-19 product has not been approved
There is sufficient evidence on all pharmacovigilance databases examined in this report to establish a concerning safety signal about Covid-19 vaccines.
Data about the Types of Adverse Reaction Reports Linked to Covid-19 Vaccines
- Data from WHO VigiAccess, EudraVigilance, and UK Yellow Card Scheme reveal that the majority of adverse events reports related to Covid-19 vaccines are: Nervous System Disorders, Musculoskeletal and Connective Tissue Disorders and Gastrointestinal Disorders
- Data from VAERS reveal that the majority of adverse event reports related to Covid-19 vaccines are: Arthritis and Arthraligia, Anaphylaxis, Venous Thromboembolism, Myocarditis/Pericarditis, Stroke, and Convulsions/Seizures
- Eudravigilance reports 1200 deaths linked to Covid-19 vaccines. UK Yellow Card reports 2100 deaths linked to Covid-19 vaccines. VAERS reports 28 000 deaths linked to Covid-19 vaccines
The types of adverse reaction reports linked to Covid-19 products are serious in nature.
Data about the Rate of Adverse Events that is Sufficient for Product Recall
- Pharmacovigilance databases, such as those examined in this report, rely on passive surveillance. Adverse events are underreported
- Covid-19 products are unique in that they were developed quickly and administered to large populations while still in Phase 3 clinical trials
- In 1976, the American government rushed a mass vaccination campaign for swine flu. Information emerged about the nature of the virus and adverse reactions linked to the vaccine, and the campaign was halted in less than a year
- Data from VAERS and FAERS reveals that The Polio Vaccine was recalled in less than 1 year after 10 reported deaths, the Swine Flu Vaccine was recalled in less than 1 year after 53 reported deaths. The Covid-19 vaccine, with over 28 000 associated reports of death, has not been recalled after two years
There is sufficient evidence of adverse events relating to Covid-19 vaccines to indicate that a product recall is immediately necessary.
Click here to download a 21-page printable PDF summary of the Covid-19 Vaccine Pharmacovigilance Report.

References
AstraZeneca. (May 2022). Case Series Drug Analysis Print: Covid-19 AstraZeneca Vaccine
Analysis Print. Gov.uk. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1080309/COVID-19_AstraZeneca_Vaccine_Analysis_Print_DLP_25.05.2022.pdf
Connor Stewart. (May 2022). COVID-19 vaccination rate in European countries. Statista.
https://www.statista.com/statistics/1196071/covid-19-vaccination-rate-in-europe-by-country/
Elflein, John. (May 2022). Vaccinations in the U.S.- Statistics & Facts. Statista.
https://www.statista.com/topics/3283/vaccinations-in-the-us/#topicHeader__wrapper
EudraVigilance. (May 2022). European database of suspected adverse drug reaction reports.
European Medicines Agency. https://www.adrreports.eu/en/eudravigilance.html#
European Centre for Disease Prevention and Control. (May 2022). COVID-19 Vaccine Tracker.
European Centre for Disease Prevention and Control. https://vaccinetracker.ecdc.europa.eu/public/extensions/covid-19/vaccine-tracker.html#uptake-tab
European Medicines Agency. (May 2022). Human regulatory: EudraVigilance. European
Medicines Agency.
https://www.ema.europa.eu/en/human-regulatory/research-development/pharmacovigilance/eudravigilance
Klein, Christopher. (Sep 2020). When the US Government Tried to Fast-Track a Flu Vaccine.
History.com. https://www.history.com/news/swine-flu-rush-vaccine-election-year-1976
Medicines & Healthcare products Regulatory Agency. (2022). Case Series Drug Analysis Print:
Covid-19 brand unspecified Vaccine Analysis Print. Gov.uk.
Medicines & Healthcare products Regulatory Agency. (2022). Research and analysis:
Coronavirus vaccine weekly summary of Yellow Card reporting. Gov.uk. https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting
Moderna. (May 2022). Case Series Drug Analysis Print: Covid-19 Moderna Vaccine
Analysis Print. Gov.uk. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1080310/COVID-19_Moderna_Vaccine_Analysis_Print_DLP_25.05.2022.pdf
OpenVAERS. (May 2022). VAERS COVID Vaccine Adverse Event Reports. OpenVAERS.
https://openvaers.com/covid-data
Pfizer-BioNTech. (May 2022). Case Series Drug Analysis Print: Covid-19 mRNA
Pfizer-BioNTech Vaccine Analysis Print. Gov.uk. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1080308/COVID-19_Pfizer-BioNTech_Vaccine_Analysis_Print_DLP_25.05.2022.pdf
Pohlman KA, Carroll L, Tsuyuki RT, et al. (2020) Comparison of active versus passive surveillance adverse event reporting in a paediatric ambulatory chiropractic care setting: a cluster randomised controlled trial. BMJ Open Quality;9:e000972. doi: 10.1136/bmjoq-2020-000972
Ritchie, Hannah; Mathieu, Edouard; Rodés-Guirao, Lucas et al. (2020). Coronavirus Pandemic
(COVID-19). Our World in Data. https://ourworldindata.org/coronavirus
Rose, Jessica. (2022). VAERS data analysis. Jessica’s Universe.
https://www.jessicasuniverse.com/blank-page-1
Thomas SJ, Moreira ED, Kitchin N et al. (2021). Safety and Efficacy of the BNT162b2 mRNA
Covid-19 Vaccine through 6 Months. New England Journal of Medicine.
https://www.nejm.org/doi/pdf/10.1056/NEJMoa2110345
Thomas SJ, Moreira ED, Kitchin N et al. (2021). Safety and Efficacy of the BNT162b2 mRNA
Covid-19 Vaccine through 6 Months – Supplementary Appendix. New England Journal of
Medicine. https://www.nejm.org/doi/suppl/10.1056/NEJMoa2034577/suppl_file/nejmoa2034577_appendix.pdf
Uppsala Monitoring Centre. (May 2022). The WHO Programme for International Drug
Monitoring (WHO PIDM). World Health Organization. https://who-umc.org/about-the-who-programme-for-international-drug-monitoring/
USA Facts. (May 2022). US Coronavirus vaccine tracker. USA Facts.
https://usafacts.org/visualizations/covid-vaccine-tracker-states/
U.S. Food & Drug Administration. (May 2022). Step 3: Clinical Research. U.S Food & Drug
Administration. https://www.fda.gov/patients/drug-development-process/step-3-clinical-research
Vaccine Adverse Event Reporting System (VAERS). (1990 – 2022). United States Department of
Health and Human Services (DHHS), Public Health Service (PHS), Centers for Disease Control (CDC) / Food and Drug Administration (FDA). CDC WONDER On-line Database. Vaccine Type and Events by Age Group. https://wonder.cdc.gov/controller/datarequest/D8;jsessionid=F9E61FE2A2B457AD46D5FC21F667
Vaccine Adverse Event Reporting System (VAERS). (2022). About VAERS.United States
Department of Health and Human Services (DHHS), Public Health Service (PHS),
Centers for Disease Control (CDC) / Food and Drug Administration (FDA). https://vaers.hhs.gov/about.html
Vaccine Adverse Event Reporting System (VAERS). (1990 – 2022). United States Department of
Health and Human Services (DHHS), Public Health Service (PHS), Centers for Disease Control (CDC) / Food and Drug Administration (FDA). CDC WONDER On-line Database. http://wonder.cdc.gov/vaers.html
VAERS Analysis Info. (May 2022). VAERS Summary for COVID-19 Vaccines. VAERS Analysis
Info.https://vaersanalysis.info/2022/05/14/vaers-summary-for-covid-19-vaccines-through-5-6-2022/
Vanderslott, Samantha; Dadonaite, Bernadeta; Roser, Max. (2013). Vaccination. Our World in
Data. https://ourworldindata.org/vaccination
VigiAccess. (1968 – 2022). Reported potential side effects. World Health
Organization Collaborating Centre for International Drug Monitoring, Uppsala Monitoring Centre. https://vigiaccess.org/
VigiAccess. (1968 – 2022). Reported potential side effects Covid-19 vaccine. World Health
Organization Collaborating Centre for International Drug Monitoring, Uppsala Monitoring Centre. https://vigiaccess.org/
VigiAccess. (1968 – 2022). Reported potential side effects Tuberculosis Vaccine. World Health
Organization Collaborating Centre for International Drug Monitoring, Uppsala Monitoring Centre. https://vigiaccess.org/
World Health Organization (web archive). (2015). Immunization, Vaccines and Biologicals:
Surveillance for Vaccine Preventable Diseases. World Health Organization. http://www.who.int/immunization/monitoring_surveillance/burden/VPDs/en/
Yellow Card. (May 2022). Coronavirus Yellow Card reporting site. Medicines & Healthcare products Regulatory Agency. https://coronavirus-yellowcard.mhra.gov.uk/
Acknowledgments
This report was drafted by Adele Paul and finalised and approved by the WCH Health and Humanity Committee.



